Chest radiograph
Chest radiographic imaging (see the images below) is an important tool in the examination of patients with an exacerbation of asthma, but patients should not be left waiting in the treatment room for a radiograph before treatment.[1] Chest radiography is the initial imaging evaluation in most individuals with symptoms of asthma. The value of chest radiography is in revealing complications or alternative causes of wheezing and the minor importance of wheezing in the diagnosis of asthma and its exacerbations. It usually is more useful in the initial diagnosis of bronchial asthma than in the detection of exacerbations, although it is valuable in excluding complications such as pneumonia and asthma mimics, even during exacerbations. Posteroanterior chest radiograph demonstrates a pneumomediastinum in bronchial asthma. Mediastinal air is noted adjacent to the anteroposterior window and airtrapping extends to the neck, especially on the right side.
Posteroanterior chest radiograph demonstrates a pneumomediastinum in bronchial asthma. Mediastinal air is noted adjacent to the anteroposterior window and airtrapping extends to the neck, especially on the right side.  Lateral chest radiograph demonstrates a pneumomediastinum in bronchial asthma. Air is noted anterior to the trachea (same patient as in the previous image). Although bronchial thickening, hyperinflation, and focal atelectasis suggest asthma when they are present, chest radiographs obtained during asthma exacerbations can demonstrate normal findings, which reduce its sensitivity as a diagnostic tool. Similarly, identical findings may be observed with chronic bronchitis and viral bronchopneumonia, among other conditions, and these similarities limit the specificity of chest radiography. Clinical correlation remains beneficial in the interpretation of findings, as it is in so many other areas of radiology.
Lateral chest radiograph demonstrates a pneumomediastinum in bronchial asthma. Air is noted anterior to the trachea (same patient as in the previous image). Although bronchial thickening, hyperinflation, and focal atelectasis suggest asthma when they are present, chest radiographs obtained during asthma exacerbations can demonstrate normal findings, which reduce its sensitivity as a diagnostic tool. Similarly, identical findings may be observed with chronic bronchitis and viral bronchopneumonia, among other conditions, and these similarities limit the specificity of chest radiography. Clinical correlation remains beneficial in the interpretation of findings, as it is in so many other areas of radiology.HRCT
High-resolution computed tomography (HRCT) is a second-line examination (see the images below). It is useful in patients with chronic or recurring symptoms and in those with possible complications such as allergic bronchopulmonary aspergillosis and bronchiectasis.[2] High-resolution CT scan of the thorax obtained during inspiration demonstrates airtrapping in a patient with asthma. Inspiratory findings are normal.
High-resolution CT scan of the thorax obtained during inspiration demonstrates airtrapping in a patient with asthma. Inspiratory findings are normal.  High-resolution CT scan of the thorax obtained during expiration demonstrates a mosaic pattern of lung attenuation in a patient with asthma. Lucent areas (arrows) represent areas of airtrapping (same patient as in the previous image).
High-resolution CT scan of the thorax obtained during expiration demonstrates a mosaic pattern of lung attenuation in a patient with asthma. Lucent areas (arrows) represent areas of airtrapping (same patient as in the previous image).  Asthma. High-resolution CT scan of the thorax obtained during inspiration in a patient with recurrent left lower lobe pneumonia shows a bronchial mucoepidermoid carcinoma (arrow). HRCT is more costly than chest radiography and exposes the patient to more radiation. Nevertheless, CT scans can demonstrate a number of findings that support the diagnosis of asthma. HRCT remains the most sensitive study for morphologic changes associated with asthma. HRCT has the potential to aid with the functional assessment of the lungs, such as tests of airtrapping and the bronchodilator response. The specificity of HRCT for bronchial asthma is limited by the similarity of its changes to those of other diseases, such as bronchiectasis, chronic bronchitis, emphysema, and bronchopulmonary aspergillosis.
Asthma. High-resolution CT scan of the thorax obtained during inspiration in a patient with recurrent left lower lobe pneumonia shows a bronchial mucoepidermoid carcinoma (arrow). HRCT is more costly than chest radiography and exposes the patient to more radiation. Nevertheless, CT scans can demonstrate a number of findings that support the diagnosis of asthma. HRCT remains the most sensitive study for morphologic changes associated with asthma. HRCT has the potential to aid with the functional assessment of the lungs, such as tests of airtrapping and the bronchodilator response. The specificity of HRCT for bronchial asthma is limited by the similarity of its changes to those of other diseases, such as bronchiectasis, chronic bronchitis, emphysema, and bronchopulmonary aspergillosis.Differential diagnosis
The aphorism attributed to Chevallier Jackson states, "All that wheezes is not asthma." This recognition suggests that imaging has an important role in differentiating asthma from its mimics and that further diagnostic evaluation and treatment of nonasthma conditions may be necessary. With his or her knowledge of the imaging findings in alternative disorders, the consulting radiologist may be valuable during the workup; he or she can recognize clinical signs and symptoms that indicate the use of high-resolution chest CT, sinus CT, CT pulmonary angiography, or MRI as the best modality for further imaging in the diagnosis.Various tracheal tumors, foreign bodies, and other conditions can contribute to wheezing. These may be misdiagnosed for several years before they are recognized.
Diffuse panbronchiolitis is prevalent in Japan and the Far East, and it may mimic bronchial asthma with wheezing, coughing, dyspnea on exertion, and sinusitis.[3] HRCT findings include centrilobular nodules and linear markings that usually are more profuse compared with the multifocal bronchiolar impaction sometimes observed with asthma.
Sinus disease, especially in children, is associated with bronchial asthma and wheezing. Although the association is not strong in patients with CT evidence of mild sinus mucosal thickening, a scoring system developed by Newman et al showed that extensive sinus disease was correlated with a substantially higher extent of wheezing than that in patients with only mild thickening.[4] Of 104 adults, 39% had extensive disease, as visualized on CT scans, which was correlated with asthma and peripheral eosinophilia.
In a Finnish study of hospital admissions for acute asthma, admission chest radiographs showed abnormalities in 50% of the patients and resulted in treatment changes in 5%. The numbers were more remarkable when a paranasal sinus series was obtained in unselected patients presented primarily because of asthma. A sinus abnormality of any kind was found in 85% of patients; maxillary sinus abnormalities occurred alone in 63%. In 29% of patients with a sinus abnormality, treatment was immediately altered. All abnormalities were identified on the Waters view alone, which is 6 times more useful than the Chest radiography in directing the treatment of acute asthma.[5] Although the findings are provocative and require confirmation, the conventional wisdom regarding the sinus radiographic evaluation of chronic coughing and asthma suggests that a workup for chronic coughing should be performed first.[6]
Cough, recurrent bronchitis, pneumonia, wheezing, and asthma are associated with gastroesophageal reflux (GER).[7, 8] The incidence of GER in those with asthma ranges from 38% in patients with only asthma symptoms to 48% in patients with recurrent pneumonia. Scintigraphic studies performed after technetium-99m sulfur-colloid ingestion have shown radionuclide activity in the lungs the next day, but no causal relationship between reflux and asthma has been established. Nevertheless, evidence suggests that increased pulmonary resistance occurs with symptoms of reflux during acid provocation testing; as some have suggested, the changes may be sufficiently significant to produce clinically evident bronchospasm.[7]
Pneumothorax may be evident radiographically before it is identified clinically.[9] It often occurs during recurrent episodes of bronchospasm, as well as in other conditions. The presence of an air-fluid level in a hydropneumothorax can be confused with pneumatocele, infected cysts, and cavitary lung disease.
For patient education information, see the Asthma Center, as well as Asthma and Asthma in Children.
Radiography
Overview
In most patients with uncomplicated asthma, radiographic findings are normal. In patients with more advanced asthma, varying stages of hyperinflation are reflected on chest radiographs by a flattening of the hemidiaphragm, increased retrosternal airspace, and relatively minor differences in diaphragmatic positions between inspiration and expiration. Other features of bronchial asthma include a mild prominence of the hilar vasculature that results from transient pulmonary hypertension and mucous plugging with or without atelectasis.[10]See the chest radiographic images below.
Posteroanterior chest radiograph demonstrates a pneumomediastinum in bronchial asthma. Mediastinal air is noted adjacent to the anteroposterior window and airtrapping extends to the neck, especially on the right side. Lateral chest radiograph demonstrates a pneumomediastinum in bronchial asthma. Air is noted anterior to the trachea (same patient as in the previous image). In early studies, lung opacity on chest radiography was evaluated in 8 regions in patients with asthma; the findings recapitulated the heterogeneous distribution of localized airtrapping seen on radioactive noble gas scintigrams obtained a decade earlier.[11] Airtrapping increases the TLC and FRC and reduces the vital capacity (VC) and inspiratory capacity (IC), where IC = TLC – FRC. FRC, which is the lung volume remaining at the end of expiration, also remains high in the patient with symptomatic asthma; this observation reflects the patient's inability to breathe out in the setting of obstructing secretions, airway narrowing, and edema.
Traditionally, the FRC and TLC have been measured in the pulmonary function laboratory, and planimetry was used in the past to assess the radiographic equivalent of the TLC. A planimeter is a mechanical device used with inspiratory posteroanterior (PA) and lateral CXRs. Formulas are used to calculate the lung volume by using a series of virtual sections in which airspace cross-sectional areas are quantified. This procedure was established as a means of diagnosing hyperinflation in bronchial asthma when correlation coefficients of 0.94 were found for helium dilution lung volumes and body plethysmography. A decrease in the TLC after treatment for asthma can be correlated with patient improvement, even when the FEV1 does not improve; this effect likely is related to an improvement in IC.[12]
The reliability of planimetry in the diagnosis of asthma in children also was established.[13] Findings from a more recent study casts doubt on the usefulness of planimetry in patients with occupational asthma.[14]
Bronchial asthma
The direct measurement of airway wall thickness with chest radiographs was undertaken in patients with mild and severe asthma and in individuals without asthma.[15] The ratio of the internal luminal diameter to the wall thickness was determined by optically measuring the bronchi, as viewed end-on on radiographs, and by reviewing plain radiographic tomograms. The measurements were compared by means of subjective assessment alone. In 11 of 15 patients with severe asthma, subjective assessment results matched the measurements.The authors stated that the finding of more than 2 measurably thickened bronchial walls was rare in individuals without asthma; however, in patients with more severe asthma, the margins of the bronchial walls were delineated better and distinguishable from the findings in individuals without asthma. Ratios varied with bronchiolar luminal diameter, and the authors believed that the ratio was more an index of chronicity than an index of severity.
Nonsegmental, widespread, streaky opacities likely represent focal linear atelectasis resulting from viral superinfection.[16] Segmental opacities may represent localized poor airway mucociliary clearance with atelectasis or early consolidation.
Radiographic correlates of increased TLC that result from airtrapping and small bronchiolar obstruction include hyperinflation; low diaphragms; and, in children, sternal bowing. Sternal bowing reportedly is present in children when the hemidiaphragms are below the 9th or 10th posterior ribs or when the dome of the diaphragm is below the 6th mid anterior rib interspace.[16] However, the value of these findings as an index of severity is disputed.[17] Hemidiaphragms may be flat or inverted, as in tension pneumothorax, and the lateral slips of the diaphragm may be observed, especially on CT scans.
Recently, observers of 65 children hospitalized for asthma noted the inversion of the pulmonary venous distribution that is typically observed in individuals with left heart failure.[18] The children tended to be younger (6.75 y vs a group mean of 9.2 y), and they had tachypnea, retractions, nasal flaring, and tachycardia. The proposed mechanism was increased intrathoracic pressure that led to right ventricular overload, paradoxical septal motion with loss of left ventricular compliance, and elevated left atrial and pulmonary venous pressures. To the authors' knowledge, this finding has not been replicated since that study, but it remains an interesting observation.
ED management
Several studies have been performed to evaluate the clinical usefulness of chest radiography.[19, 20, 21, 22, 16, 23, 24, 25, 26, 25, 27, 28, 29, 30, 31]In a study of 117 patients with asthma who were older than 15 years, hyperinflation and bronchovascular changes were seen on chest radiograph in 31% of patients in whom asthma began before they were aged 15 years. However, these changes were not observed in any patients in whom asthma began after they were aged 30 years.[19]
In a study of outpatients with acute asthma who present to an emergency department (ED), a mean of 55% of patients had normal radiographic findings, while 37% had findings of hyperinflation, and 7% had minimal and unchanged interstitial abnormalities.[20] Pneumonia was present in 16% of adults. Despite the large statistical range of patients with only normal findings (30-81%) and despite the discovery of pneumomediastinum in 5% of children, the authors concluded that chest radiography was not helpful unless complications of asthma were suggested clinically.
One of the largest studies of ED visits involving CXRs was performed in a large city hospital. In this study, findings in 5,000 patients were reviewed; 2-view radiographs used in two thirds of the patients and only portable radiographs were used in one third. Overall, 35% of the patients with chest symptoms had serious radiographic findings, but only 14% of the patients with symptoms of asthma had serious radiographic abnormalities. However, the applicability of these findings to individual CXR findings of asthma is limited by the small proportion of total radiographs (4.6%) obtained in patients with asthma.[24]
In a British general hospital ED, findings in 695 episodes of acute asthma in adults and children were evaluated. CXRs were obtained in 135 of 695 patients, or 19% of the total instances of asthmatic exacerbation. Of the radiographs, 79% (presumably portable radiographs) demonstrated normal findings. Abnormalities included evidence of infection (13%), hyperinflation (7%), and edema (2%). Increased perihilar markings were observed in only 2 patients.[28]
Hospital admission
In an early study, the value of routine admission radiography in adults with asthma was evaluated in regard to the presence of pneumonia in patients with acute respiratory complaints. Among patients with asthma, only 2% had concurrent pneumonia.[23] .Sherman et al examined patients with exacerbations of chronic obstructive airway disease (COPD). More than half of the 242 hospitalized patients had a "predominant clinical pattern of asthma." Wheezing was not specifically listed as a clinical finding for any patient, although cough and dyspnea were included. Only 4.5% of the radiographs resulted in clinically significant findings that changed the treatment planned with clinical and laboratory criteria alone, in the asthma group as well as the whole group.
Sherman et al[26] concluded that admission chest radiography is justified only after the following selection criteria are met: WBC more than 15 X 109/L; polymorphonuclear count more than 8 X 109/L; or a history of congestive heart failure, coronary artery disease, chest pain, or edema. The findings affirmed the observation that chronic bronchitis and emphysema can have a presentation similar to that of bronchial asthma. This result is notable because it came in one of the earlier studies that did not find value with routine CXR in the ED for patients with asthma.
In a blinded retrospective review, the effect of chest radiography on clinical decision making, including those related to hospital admission, was evaluated in a busy large-city ED.[25, 30] Criteria for complicated airway disease included COPD, fever, heart disease, intravenous drug abuse, immunodeficiency, and/or prior thoracic surgery but not diabetes or steroid use. Of the 27 patients in whom treatment was altered, 96% had clinically and radiographically complicated cases. Abnormal radiographic features that were influential in the clinical input included infiltrate in 63%, congestive heart failure in 26%, and lobar collapse in 4%. Features of uncomplicated CXRs were peribronchial thickening in 18% and atelectasis and other findings in fewer than 10%. Had the stated criteria for complicated asthma versus uncomplicated asthma been applied, chest radiographic examinations for hospital admission would have decreased by an estimated 34%.
In another study, more than 85% of patients underwent 2-view radiographs; in earlier studies, a lower proportion of PA and lateral examinations were performed relative to portable anteroposterior (AP) studies.[26]
White et al prospectively studied admission chest radiographs in a large-city ED. PA and lateral radiographs were obtained in more than 95% of the patients who eventually were admitted after a 12-hour course of treatment. Major findings, present in 34% of the patients, included focal opacity, increased interstitial markings, cardiomegaly, pulmonary venous congestion, pneumothorax, and new pulmonary nodules. Minor findings, present in 41%, included hyperinflation, pleural thickening, and calcified granulomas. Focal opacities or increased interstitial markings were correlated with subsequent antibiotic use, independent of an elevated WBC or body temperature. The authors concluded that CXRs should be obtained in all adult patients with acute asthma who are admitted.[27]
Pediatric asthma
In children, the natural overlap of nonbacterial bronchiolitis with bronchial asthma accounts for their similar findings on radiographs. Findings of an increased retrosternal airspace and flattened hemidiaphragms sometimes are accompanied by peripheral arterial attenuation. These findings are components of the hyperinflation observed with both entities.[32]A study of 371 children with first-time wheezing led to the establishment of criteria for obtaining chest radiographs.[22] The criteria include a heart rate higher than 160 bpm or a respiratory rate higher than 60 per minute, localized rales or localized decreased breath sounds before treatment, and/or persistent localized rales and localized wheezing after treatment. Patients are more likely to have significantly positive chest radiographic findings when criteria are met. Of children with abnormal radiographic findings of segmental atelectasis, pneumonia, and pneumomediastinum, 95% met the prospective criteria. However, negative findings still included hyperinflation, thickened airways, peribronchial thickening, and subsegmental atelectasis.
Roback et al also evaluated the use of chest radiography in children with first-time wheezing by using the practice parameters of Gershel et al as a yardstick with which to compare actual clinical practice. The retrospective study revealed that, of the 41% of the patients who underwent chest radiography, 24% had a clinically significant abnormality such as local consolidation, pneumothorax, pneumomediastinum, asymmetric opacity, hyperinflation, segmental atelectasis, edema, cardiomegaly, or airway compression.[31]
In the study of Roback et al,[31] an elevated temperature (mean, 37.9°C), absence of a family history of asthma, localized wheezes, decreased breath sounds, and rales significantly predicted the decision to perform chest radiography. Patients in whom chest radiography was performed (67%) were more likely to have positive findings when they had a slightly elevated temperature, a family history of asthma, or localized wheezes or rales. Of patients in whom chest radiography was not performed, 62% would have undergone radiography with the criteria of Gershel et al. Of patients who underwent radiography, 74% did not meet these criteria; this finding suggests that the criteria and actual clinical practice widely differ.
A more recent study of pediatric asthma examined children with first-time wheezing who presented to the ED in a large-city children's hospital. On the radiographs obtained in these children, 61% showed findings of uncomplicated bronchiolitis or asthma (hyperinflation in 85%, peribronchial cuffing in 68%, interstitial or perihilar opacities in 31%, and atelectasis), and 18% showed parenchymal opacities (lobar or segmental). Only 21% of patients had completely normal radiographic findings.
Rubenstein et al[29] compared the usefulness of routine spirometry with that of chest radiography in patients with mild ambulatory asthma in a university student population. Although 36% of the patients had spirometric results consistent with airway obstruction (predicted FEV1 < 80%, predicted peak expiratory flow rate [PEFR] < 85%, or 20% improvement with bronchodilators), 59% had abnormal radiographic findings consisting of hyperinflation, increased perihilar markings, and peribronchial or peribronchiolar cuffing. Bronchitis and/or bronchiolitis and bronchial asthma caused the radiographic findings. Thus, although chest radiography lacks optimal specificity, it may be valuable in the diagnosis of bronchial asthma when the clinical features were taken into account.
Bronchography
Bronchography is a technique, now largely archaic, that is used to visualize the trachea and large airways by instilling a radiopaque, oily emulsion into the airways via an airway catheter or bronchoscope. For many years bronchography, was a criterion standard in the detection of bronchiectasis, but bronchography was known to induce transient bronchospasm and impair ventilation and diffusion capacity, especially in individuals with asthma. Typically, bronchography was considered contraindicated in severe reactive airway disease, although it was useful in the examination of individuals with milder asthma with suspected bronchiectasis.[33]A group from Finland used cinetracheobronchography to visualize the main airways in individuals with asthma. The investigators introduced bronchography contrast enhancement and performed radiography during the patient's quiet breathing, forced expiration, and coughing.[34] The authors described findings in a patient in whom complete closure of the distal trachea during coughing was associated with both cartilaginous and membranous weakening. The patient's condition responded to endobronchial prosthesis with a marked improvement in airflow and symptoms.
In dogs, tantalum bronchography was performed in studies of experimental asthma at the Cardiovascular Research Institute during the 1960s and 1970s. Tantalum fine powder was insufflated into the bronchi, and it allowed detailed study of airways in asthma caused by various pharmacologic agents with and without bronchial provocation by allergens and particulates.
In one study, nematode antigen caused airway narrowing of differing degrees, according to airway size. Airways sized 1- to 8-mm had the greatest diameter decrease (49%) compared with airways with diameters greater than 12 mm, 8-12 mm, or 0.5-1.0 mm. Although it is not entirely inert, the stimulation of increased respiratory system resistance by the antigen is controlled by the dose.[35]
Nematode antigen was used to evaluate airway narrowing in some patients with asthma. The advantage of the metallic powder is its relatively inert character in the airways, although it is known to affect mucociliary clearance to a small degree.[36] The agent was used to study the somewhat twitchy airways of patients with asthma, in contrast to the more noxious, typical, oil-based, iodinated suspensions that are commonly used for bronchography.
Computed Tomography
Overview
The role of computed tomography (CT) in the imaging of airway disease increased after the development of lung high-resolution CT (HRCT). The technical progress of thin-section acquisition, high-spatial-frequency data reconstruction (ie, bone algorithm technique), and targeted reconstruction has allowed the visualization of finer details on HRCT scans; these details include airtrapping, measurable bronchial wall thickening, atelectasis, centrilobular nodules due to mucous plugging, and acinar nodules due to low-grade inflammatory changes.[37, 38, 39]King et al discuss details of HRCT methods for evaluating the airways in obstructive pulmonary disease.[40] They discuss the technical features of HRCT and review its use in the assessment of obstructive airway disease.
See the asthma-related HRCT images below.
High-resolution CT scan of the thorax obtained during inspiration demonstrates airtrapping in a patient with asthma. Inspiratory findings are normal. High-resolution CT scan of the thorax obtained during expiration demonstrates a mosaic pattern of lung attenuation in a patient with asthma. Lucent areas (arrows) represent areas of airtrapping (same patient as in the previous image). Asthma. High-resolution CT scan of the thorax obtained during inspiration in a patient with recurrent left lower lobe pneumonia shows a bronchial mucoepidermoid carcinoma (arrow). 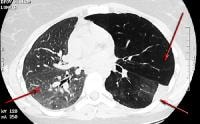 Asthma. High-resolution CT scan of the thorax obtained during expiration in a patient with recurrent left lower lobe pneumonia shows a bronchial mucoepidermoid carcinoma (same patient as in the previous image). Note the normal increase in right lung attenuation during expiration (right arrow). The left lung remains lucent, especially the upper lobe, secondary to bronchial obstruction with airtrapping (left upper arrow). The vasculature on the left is diminutive, secondary to reflex vasoconstriction. Left pleural thickening and abnormal linear opacities are noted in the left lower lobe; these are the result of prior episodes of postobstructive pneumonia (left lower arrow).
Asthma. High-resolution CT scan of the thorax obtained during expiration in a patient with recurrent left lower lobe pneumonia shows a bronchial mucoepidermoid carcinoma (same patient as in the previous image). Note the normal increase in right lung attenuation during expiration (right arrow). The left lung remains lucent, especially the upper lobe, secondary to bronchial obstruction with airtrapping (left upper arrow). The vasculature on the left is diminutive, secondary to reflex vasoconstriction. Left pleural thickening and abnormal linear opacities are noted in the left lower lobe; these are the result of prior episodes of postobstructive pneumonia (left lower arrow).  Asthma. High-resolution CT scan of the thorax demonstrates mild bronchial thickening and dilatation in a patient with bilateral lung transplants and bronchial asthma.
Asthma. High-resolution CT scan of the thorax demonstrates mild bronchial thickening and dilatation in a patient with bilateral lung transplants and bronchial asthma.  Asthma. High-resolution CT scan of the thorax demonstrates central bronchiectasis, a hallmark of allergic bronchopulmonary aspergillosis (right arrow), and the peripheral tree-in-bud appearance of centrilobular opacities (left arrow), which represent mucoid impaction of the small bronchioles.
Asthma. High-resolution CT scan of the thorax demonstrates central bronchiectasis, a hallmark of allergic bronchopulmonary aspergillosis (right arrow), and the peripheral tree-in-bud appearance of centrilobular opacities (left arrow), which represent mucoid impaction of the small bronchioles. 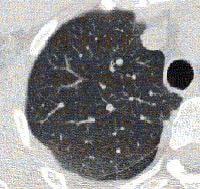 Baseline high-resolution CT scan of the thorax obtained during expiration in a patient with bronchial asthma.
Baseline high-resolution CT scan of the thorax obtained during expiration in a patient with bronchial asthma. 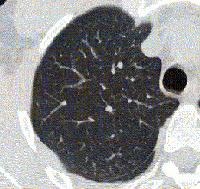 Asthma. High-resolution CT scan of the thorax obtained during expiration and after a methacholine challenge in the same patient as in the previous image. Note the greater degree of airtrapping in the posterior subpleural aspects of the right upper lobe after methacholine is administered.
Asthma. High-resolution CT scan of the thorax obtained during expiration and after a methacholine challenge in the same patient as in the previous image. Note the greater degree of airtrapping in the posterior subpleural aspects of the right upper lobe after methacholine is administered. Animal studies
In one study, the intact lobes of pressurized canine lungs were evaluated with HRCT before and after the administration of carbachol, a bronchoconstrictor. Intermediate-sized airways had the most prominent decreases in luminal area; 2- to 4-mm airways had a 56% reduction in diameter, and 4- to 6-mm airways had a 59% reduction. Wall thickening was believed to result, in part, from increased bronchial blood flow, edema, and smooth muscle hyperplasia. The lower range of visibility was at the generally accepted maximal diameter of small airways, that is, 2 mm.[41]Herold et al established the usefulness of HRCT in measuring the bronchial response to bronchoconstrictors in the setting of hyperreactivity. Responses to aerosol isotonic sodium chloride solution and histamine were assessed in anesthetized ventilated dogs and corrected for lung volume. Airway cross-sectional area decreased by 43% after histamine administration and by 26% after saline administration alone, but intersubject and intrasubject variability was significant; the irritant effect of the base aerosol was evident. Although airways as small as 1 mm were evaluated, the discrepancy between the response of large airways (ie, bronchoconstriction) and small airways (ie, change in mean airway pressure) could not be explained.[42]
The role of vascular engorgement and edema was evaluated with HRCT. Dogs received 3 successive 50 mL/kg isotonic sodium chloride challenges or 2 successive 25 mL/kg blood infusions. This large sodium chloride load caused more airway wall thickening and luminal narrowing than blood alone. With sodium chloride, the luminal area and wall thickness were 68% and 150% of those at baseline, respectively; with blood, the results were 81% and 108% of those of baseline, respectively. The findings were not reversible within 30 minutes. Also, the findings were attributed to edema in airway walls, but they were considered to have only a minor role in the multiple causes of increased airway resistance in asthma and left ventricular dysfunction.[43] .
The investigators then showed that, although the initial histamine challenge narrowed the airways to 71% of their baseline luminal area, the sodium chloride challenge alone (100 mL/kg) reduced the airway lumen to 78% of its baseline size. Potentiation of the effect by combining sodium chloride and histamine reduced the luminal area to 54% of its baseline value. These findings were correlated with the known exaggerated constrictor response to provocation in the setting of airway edema[44] .
Findings from later studies of the role of inflammatory mediators in airway hyperresponsiveness led to the conclusion that methacholine and bradykinin, alone or combined, have only minor effects on bronchoconstriction[45]
Bronchial asthma
HRCT findings in bronchial asthma include the following:- Bronchial wall thickening
- Bronchial dilatation
- Cylindrical and varicose bronchiectasis
- Reduced airway luminal area
- Mucoid impaction of the bronchi
- Centrilobular opacities, or bronchiolar impaction
- Linear opacities
- Airtrapping, as demonstrated or exacerbated with expiration
- Mosaic lung attenuation, or focal and regional areas of decreased perfusions
Emphysema and airtrapping
Some initial human studies involved emphysema scoring in patients with asthma. Royle first described emphysema in severe asthma by using radiographs in current or former smokers.In the late 1980s, a group evaluated the coexistence of emphysema and asthma findings using HRCT. In comparing 10 nonsmoking patients with asthma with 10 matched cigarette smokers with severe airflow obstruction, an emphysema grade of 0% was observed in the nonsmokers, and 100%, in smokers; the emphysema score reflected vascular disruption, bullae, and low-attenuating areas. Although all smokers with a TLC greater than 120% had at least some emphysema, no nonsmoking patients with asthma had emphysema. The authors concluded that, in patients with asthma, elevated TLC between attacks can be explained by hyperinflation, which is entirely due to asthma and not coexisting emphysema.[46]
Paganin et al studied airway remodeling in nonsmokers with allergic asthma and in those with nonallergic asthma. On HRCT scans, the authors observed emphysema, cylindrical and varicose bronchiectasis, bronchial wall thickening (ie, bronchial recruitment), and linear opacities ("sequellar line shadows"). The findings were significantly more prevalent in individuals with nonallergic asthma than in individuals with allergic asthma. Scores of the findings were significantly greater in both groups and were associated with the severity and duration of asthma.[47] Centrilobular emphysema was most severe in individuals with severe nonallergic asthma and was not observed in control subjects without asthma.
Whether true emphysema exists in patients with asthma or whether only terminal airspace enlargement is involved in bronchial asthma.[48] the severity of the findings appears to be correlated with the clinical measures of severe asthma. Paganin et al suggested that some form of airway remodeling accounted for the findings and that the process likely differed in allergic asthma versus nonallergic asthma. An interesting speculation is that interstitial emphysema and peribronchial fibrosis may be the result of rupture of the dilated bronchial glands that are present in bronchial asthma.[49]
Confirming earlier findings, authors from Japan also showed that smokers with moderately severe asthma have a significantly higher emphysema score (13.7% vs 2.3%) than that of nonsmokers. As expected, the diffusion capacity was correlated with the emphysema score and the pack-years of cigarette smoking. The authors concluded that, in smokers with asthma, emphysema develops independent of the asthmatic condition.[50] Determining the difference between the 2 conditions may illuminate variations in the decline of lung function and the prognosis.
The 10-year mortality rate in patients with an emphysematous form of COPD (ie, 60%) is substantially worse than that of atopic control subjects or nonsmokers with known asthma (15%).[51, 52] Therefore, differentiating between the 2 groups is important from an imaging point of view.
Findings of a later study confirmed that a subgroup of individuals with asthma who also had emphysema tended to smoke more than others and that they have poorer lung function.[53] In this study, the patients with asthma were selected from a group with suspected allergic bronchopulmonary aspergillosis (ABPA) who actually did not have ABPA, cystic fibrosis, bronchiectasis, or immune deficiency, as prior laboratory and HRCT findings revealed.
In another study, a group of individuals with reversible asthma were stratified in terms of absent, mild, or severe emphysema. Neither the duration nor the severity of asthma was correlated with the presence of emphysema, whereas smoking history, sex, and age were strongly correlated. Patients with long-standing and partially reversible bronchial asthma did not have emphysema if they were nonsmokers.[54] The findings also were consistent with the observation that DLCO typically is preserved in nonsmokers with asthma.
The correlation of airtrapping with pulmonary function was studied by using HRCT in 74 patients with chronic airway disease, including asthma,[55] and it was found that on expiratory HRCT scans, the airtrapping and expired volume scores were inversely correlated with FEV1, FEV1/FVC, and FEF25. The TLC was not correlated with any of the imaging, age, sex, cigarette smoking history, or visual HRCT scores. Airtrapping was found, even when PFT results were normal; this finding suggests a complementary role for HRCT in the functional evaluation of asthma. HRCT may be more sensitive than PFT or DLCO alone in the evaluation of centrilobular and panlobular emphysema.[49]
By the late 1980s, the HRCT features that were accepted as demonstrating emphysema included low-attenuating regions, pulmonary vascular pruning, distortion, disruption, and bullae. The use of an attenuation mask allowed the semiautomated measurement of hypoattenuation in focal regions of the lungs, with quantification in regions of interest, in which other findings then were correlated.[56]
Gevenois et al demonstrated that the distribution of lung attenuation, as visualized on CT scans, depends on the TLC and, to a lesser degree, age.[57] However, Biernacki et al showed a considerable overlap in lung attenuation, as measured in Hounsfield units, in the evaluation of patients with chronic asthma, patients with chronic bronchitis and emphysema, and control subjects without asthma. The authors confirmed a correlation (r = 0.63) between TLC and the index of lung attenuation, although neither lung attenuation nor TLC changed after PEFR improved with the use of a nebulized adrenergic bronchodilator.[58]
Ng et al investigated airtrapping as an expression of small airway narrowing. The authors examined 106 patients with small airway disease and 19 healthy individuals. They found that decreased attenuation was more prominent on expiratory HRCT scans than on inspiratory HRCT scans.[59]
Quantitative CT analysis also has promise. Newman et al demonstrated that patients with asthma could be distinguished from individuals without asthma by using machine calculations of the percentage of lung area near the diaphragm with an attenuation less than –900 HU at end expiration.[60] This finding was true for both standard CT and HRCT, and it was correlated with the degree of airtrapping, as measured with the FRC and RV. A report of expiratory HRCT findings of airtrapping included inspiratory scans that had normal findings and suggested that the most common underlying causes of airtrapping were asthma and bronchiolitis obliterans.[61]
Additional methods have emerged with the development of dynamic HRCT scanning. With these methods, anatomic variations in bronchial obstruction can be studied after a provocative challenge. For example, the temporal development of airtrapping can be demonstrated with the successive, rapid acquisition of CT images during expiration.[62] .
Dynamic CT scans demonstrate that the increase in attenuation in the dependent and basilar portions of the lungs in individuals without asthma is greater than that of individuals with asthma.[63] Nevertheless, images in 4 of 10 individuals without asthma also showed airtrapping during rapid exhalation. Clinically, the usefulness of this modality is yet to be determined.
Bronchiectasis and bronchial dilatation
Studies of HRCT images in asthma consistently reveal the presence of bronchiectasis in patients with asthma but not ABPA. In ABPA, bronchiectasis often is considered part of the definition of the disease. Dilated airways may take the form of cylindrical, varicose, or cystic bronchiectasis. Park et al observed bronchial dilatation in 31% of patients with asthma versus 7% of control subjects. The authors measured bronchoarterial ratios but did not find a statistically significant difference between the groups.[64]Lynch et al showed that dilated bronchi, defined as bronchi that are larger than accompanying arteries in which the tapering pattern is not lost, were observed in 59% of the control subjects compared with 77% of the patients with asthma. Other researchers found no or few such features in control subjects. A decreased arterial diameter with hypoventilation and hypoxic vasoconstriction, a sectioning artifact near the branching arteries and bronchi, a bronchodilator effect on medium-sized airways, and subclinical ABPA are potential explanations for the unexpectedly high percentage of findings in control subjects. The authors discussed CT scanner gantry tilting, as used in HRCT examination of patients with bronchiectasis.[65] They outlined their ability to follow the natural branching pattern of the bronchi in their plane.[53]
The reported prevalence of dilated, normally tapering bronchi ranged from 18% with skin test results that were positive for Aspergillus species, which are common in patients with mild asthma, to almost 80% in patients with moderately severe asthma. The varicose type, observed in as many as 60% of patients, was considered to be more specific for nonallergic asthma and severe asthma, whereas the cylindrical type occurred in both allergic asthma and nonallergic asthma with varying degrees of severity.[47]
In a study by Grenier et al, subsegmental and distal bronchiectasis was more common in patients with asthma (29%) than in healthy volunteers (7%). The changes were considered permanent, especially if they were varicose or cystic; the prevalence of these changes and the number of involved lobes increased with disease severity. The authors studied interobserver variability and found that interobserver and intraobserver agreement (k = 0.40) were clinically acceptable for bronchial wall thickening, bronchial dilatation, small centrilobular opacities, and decreased lung attenuation. Interobserver and intraobserver agreement was not clinically acceptable with subtypes of bronchiectasis, such as the cylindrical and varicose subtypes.[66]
Investigators in early studies used HRCT findings to prove that bronchial dilatation was prevalent in 41% of the pulmonary lobes in 8 patients with asthma who had clinical and immunologic evidence of ABPA and in 15% of lobes studied in 8 patients with asthma who had positive skin test results for only Aspergillus fumigatus.[33] The authors speculated that the unexpected findings in individuals with asthma alone may have been due to steroidal suppression of immunologic markers in these patients who actually had ABPA, non-Aspergillus fungal disease, or cylindrical bronchiectasis.
Although upper lobe involvement and bronchial wall thickening were considered nonspecific findings, Neeld et al raised the awareness that asthma may be more destructive than previously thought. Also, central bronchiectasis in its various forms primarily may reflect the duration of an inflammatory airway process rather than determine the difference between ABPA and asthma per se.[33]
Compared with the value of the traditional modality of bronchography, the value of thoracic HRCT in demonstrating central bronchiectasis in ABPA was proven in all 21 patients with the disease and in most of the segments. Central and peripheral bronchiectasis, but not peripheral bronchiectasis alone, have been evaluated by using both chest radiography and HRCT images as a diagnostic criteria for ABPA. Angus et al observed bronchial dilatation in 82% of their 17 patients and in 41% of the affected lobes in patients with ABPA versus 18% and 5%, respectively, in patients with asthma and in those without ABPA. However, peripheral bronchiectasis alone was not found in any of the patients with ABPA.[67]
Mucoid impaction is a well-defined finding in patients with ABPA. It may appear as centrilobular bronchiolar plugging or have a tree-in-bud appearance on HRCT scans. Mucoid impaction is believed to be one of the physiologic origins of mosaic lung attenuation.[10] Paganin et al attributed the development of varying degrees of cylindrical bronchiectasis to sequela of multifocal mucoid impactions and bronchial hypersecretion in asthma[47]
Grenier et al found a 21% incidence of centrilobular opacities on HRCT scans obtained in patients with asthma, compared with 5% in individuals without asthma. The authors believed that these opacities and the decreased lung attenuation can be related to the severity of asthma. The authors studied intraobserver and interobserver variability and found that, with bronchial wall thickening, bronchial dilatation, small centrilobular opacities, and decreased lung attenuation, intraobserver (k = 0.60-0.79) and interobserver (k = 0.40-0.64) agreement was clinically acceptable.[66]
Bronchial wall thickening
Carroll et al found that, in cartilaginous airways, the total areas of the inner wall and outer wall, smooth muscle, mucous gland, and cartilage were greater in fatal cases of asthma than in control and nonfatal cases.[68] The internal size of segmental to sixth-generation bronchi was studied in healthy control subjects by using HRCT. Measurements ranged from 0.8-8 mm in diameter, with the use of 2-HU windows, 5X optical magnification, and automated luminal area calculation. The authors used a 2-HU window to clarify the edges of the bronchial walls to enhance the reproducibility of the measurement.[69]Hudon et al used HRCT to show that bronchial thickening in patients with asthma and irreversible airflow obstruction was significantly greater (2.4 mm) than that of patients with completely reversible asthma (2 mm) despite the similar internal diameters of their airways.[70]
Lynch et al observed bronchial wall thickening on CXRs and HRCT scans in 71% and 92% of individuals with asthma, respectively (vs HRCT in 19% of control subjects). The authors' patient selection was somewhat biased toward those with asthma complications and smokers (44%).[53] As discussed before, a decreased arterial diameter with hypoventilation and hypoxic vasoconstriction, a sectioning artifact near branching arteries and bronchi, a bronchodilator effect on medium airways, and subclinical ABPA were considered to be potential explanations for the unexpectedly high percentage of findings in control subjects.
Park et al found bronchial wall thickening proportional to severity in 44% of stable nonsmokers with asthma versus 4% of control subjects. Bronchial wall thickening occurred in 83% of patients with severe airflow obstruction versus 35% in patients with mild obstruction and 38% in control subjects.[64]
Grenier et al found bronchial wall thickening in 82% of patients with asthma versus 7% of control subjects; this finding established one of the largest differentials between these groups, although the measurements were solely subjective. Nevertheless, the method of measurement appeared to be reliable in terms of intraobserver and interobserver variability.[66] Others had similar findings.[67, 71, 47, 72]
In an autopsy study of individuals who died with asthma as well as those who died from asthma, large airway and small airway thickening was observed in individuals with lethal asthma, whereas small airway thickening was observed only in nonlethal asthma.[68]
Awadh et al studied airway wall thickening and found no significant difference in the ratio of wall thickness to outer diameter or the percentage of wall area to the total outside cross-section in patients with near-lethal asthmatic attacks versus patients with moderate asthma.[73] Both groups differed from patients with mild asthma and from individuals without asthma. Nevertheless, even the group with mild asthma differed from individuals without asthma; this finding confirming those of others and demonstrating that individuals with mild asthma can have airway thickening if the condition is chronic. The findings were present in both the small airways (< 2 mm) and the larger airways (>2 mm). The findings support the concept of chronic airway thickening in asthma and the likelihood of airway remodeling; interstitial peribronchial fibrosis; and, perhaps, parabronchial inflammation, which may cause accompanying centrilobular emphysema.
Bronchial responsiveness
Okazawa et al evaluated a known feature in patients with asthma, that is, the exaggerated airway response to bronchoconstricting stimuli. Patients with mild-to-moderate asthma and control subjects received a methacholine challenge, and airway lumen narrowing was normalized for FRC. In both groups, the site similar (small, < 2 mm; medium, >2 mm) and extent of airway luminal narrowing on HRCT scans were similar, as were the reductions in FEV1 values. Only patients with asthma had extensive small airway wall thickening without an increased airway wall area; this finding did not change much after a bronchoconstrictor was administered. Control subjects did not have wall thickening, and their airway wall area decreased. The authors concluded that nonreversible small airway wall thickening in patients with asthma contributed to an exaggerated response of the small airways to stimuli.[74]In the intermediate bronchi of individuals with asthma and fixed or partly reversible obstruction, Boulet et al observed no difference in bronchial wall thickness relative to the diameter compared with that of control subjects. Small airways, in which asthma and COPD cause substantial pathophysiologic changes, were not studied. The authors suggested that mechanical properties of the airway wall were probably more important than wall thickness in determining airway responsiveness.[75]
In another study of bronchoeffector agents, the appearance of the airways on HRCT scans showed that airway internal luminal diameter slightly decreased in individuals with mild asthma and that specific airway resistance increased after methacholine administration; this effect completely reversed after the bronchodilator agent albuterol was administered, and an improvement compared with baseline values was even observed. Airway wall thickness did not change in terms of the diameter, and pulmonary functions did not change with treatment. The investigators were able to quantify the changes in patients with asthma and control subjects by using HRCT scans.[76]
In attempting to differentiate COPD from asthma with HRCT scans, Park et al showed that bronchial walls were thicker in bronchial asthma (2.3 mm thicker than normal) than in COPD (0.9 mm thicker than normal). However, the ratio of wall thickness to luminal diameter was not correlated with clinical features such as smoking history, duration of symptoms, physiologic measures (eg, FEV1), specific airway conductance, and a provocative concentration of the bronchoconstrictor methacholine. HRCT findings of tubular bronchiectasis, emphysema, and mosaic lung attenuation were correlated with a long history of asthma symptoms, compromised lung function, and decreased bronchial hyper responsiveness.[64] The authors concluded that differentiating COPD from asthma is possible from the data, although the usefulness of the data in individual cases remains speculative.
Carr et al studied the role of the small airways in severe asthma by using HRCT. Inspiratory and expiratory scans were obtained with an electron-beam scanner. The mean decrease in the expiratory-to-inspiratory cross-sectional area was measured: Findings were 76% in patients versus 45% in control subjects. The results showed marked initial inspiratory airway narrowing, and further narrowing with expiration in patients with asthma was limited. The authors also found that FEV1 was correlated with this narrowing and with CT features of airtrapping, but not with features of airway wall thickening or airway dilatation. Airtrapping was observed with and without overt bronchiectasis in some lung regions; this finding led to the speculation that small airway disease with airtrapping may precede bronchiectasis. As previously shown, FEV1 and RV are correlated with end-expiratory airtrapping in individuals with asthma.[77]
Guckel et al also evaluated the source of mosaic attenuation on HRCT scans and observed the influence of oxygen administration on this appearance. In 22 patients with asthma who received a methacholine challenge, high-flow oxygen administered by face mask at a rate of 12 L/min produced the greatest increase in volume-corrected attenuation in regions of mosaic attenuation, compared with the nasal administration of oxygen at a rate of 5 L/min or the use of room air. The proposed and plausible explanation is that hypoxic vasoconstriction, another known cause of mosaic attenuation (airtrapping) besides bronchial narrowing, may account for foci of decreased attenuation in patients with asthma.[78]
In addition, airtrapping is observed in some areas of bronchiectasis in individuals with asthma due to weakness of the bronchiolar walls and resultant airway collapse during exhalation.[79] Ng et al investigated airtrapping as an expression of small airway narrowing on HRCT scans. The authors examined 106 patients with small airway disease and 19 healthy individuals. They found that decreased attenuation was more prominent on expiratory HRCT scans than on inspiratory HRCT scans.[59]
Effect of treatment
Paganin et al found both reversible and irreversible findings on HRCT scans of individuals with asthma. Mucoid impaction, acinar opacities, and lobar collapse resolved within 2 weeks of treatment with oral steroids. Bronchiectasis, bronchial wall thickening, linear opacities, and emphysema were unchanged during that interval and were considered permanent. While chest radiographs alone showed abnormal findings in 38% of patients, CT demonstrated abnormal findings in 72% of patients, and the authors concluded that patients with more severe asthma are more likely to have irreversible abnormalities.[71]Grenier et al also studied the effect of treatment in patients with asthma without ABPA who had more mucoid impaction or lobar collapse on HRCT scans than on chest radiographs alone. The features tended to resolve with use of corticosteroids.[66]
Another study of bronchoeffector agents and the appearance of airways on HRCT scans revealed that airway internal luminal diameter slightly decreased and specific airway resistance increased after the administration of methacholine in patients with mild asthma. These effects completely reversed after the bronchodilator agent albuterol was administered, and an improvement compared with baseline values was even observed. Airway wall thickness did not change with treatment in these patients or in the control subjects. In the control subjects, neither airway luminal diameter nor pulmonary function changed. HRCT scans significantly aid in quantifying the changes in patients with asthma and in control subjects.[76]
Goldin et al examined 15 patients with asthma and 8 control subjects by using spirometry and HRCT and by using a methacholine challenge and albuterol inhalant reversal (see the images below). The authors showed a shift in the frequency distribution curve of lung attenuation and small airway cross-sectional area after bronchoprovocation; the findings reversed after bronchodilators were administered. The findings were correlated with changes in FEV1 in individuals with asthma and with a lack of changes in control subjects.[80]
Baseline high-resolution CT scan of the thorax obtained during expiration in a patient with bronchial asthma. Asthma. High-resolution CT scan of the thorax obtained during expiration and after a methacholine challenge in the same patient as in the previous image. Note the greater degree of airtrapping in the posterior subpleural aspects of the right upper lobe after methacholine is administered. 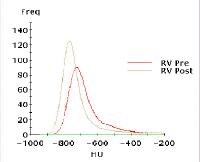 Asthma. Graph demonstrates results in right upper lobe matched pairs before and after a methacholine challenge. The resulting frequency distribution of regional lung density in the midright upper lobe demonstrates a leftward shift to lower attenuation after methacholine administration. Courtesy of Jonathan Goldin, MD, University of California, Los Angeles.
Asthma. Graph demonstrates results in right upper lobe matched pairs before and after a methacholine challenge. The resulting frequency distribution of regional lung density in the midright upper lobe demonstrates a leftward shift to lower attenuation after methacholine administration. Courtesy of Jonathan Goldin, MD, University of California, Los Angeles. Magnetic Resonance Imaging
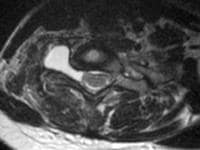
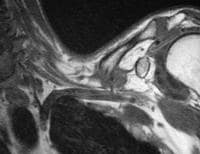
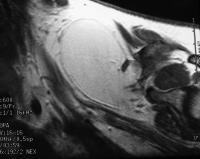
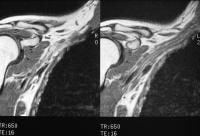
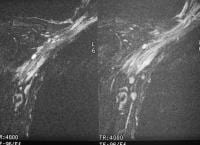
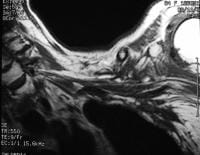
Aside from cardiovascular applications, MRI of the thorax is used primarily as a problem-solving modality in the workup of patients with lung, mediastinal, or pleural lesions. MRI is a useful alternative to CT pulmonary angiography in evaluating possible pulmonary embolic disease in patients in whom iodinated contrast agent cannot be administered and when the avoidance of ionizing radiation is preferred. In bronchial asthma, the most promising work appears to involve the use of special paramagnetic gases, which amplify the low signal-to-noise ratio of conventional spin-echo and gradient-echo techniques by several thousand times. The use of such gases offsets the disadvantages of the large magnetic susceptibility states with consequent shortened T2* signals induced by the air-alveolar interfaces.Using hyperpolarized helium (3 He) produced as needed in a local laser laboratory, de Lange and colleagues performed 32 MRI examinations with a 2-dimensional fast low-angle shot (FLASH) sequence and an interleaved echo-planar sequence immediately after the patient inhaled 1-2 L of freshly prepared gas. The imaging required short-to-intermediate breath holds (approximately 5-22 s), a set of Helmholtz coils centered over the anterior and posterior thorax, and a special radiofrequency receiver tuned to the 48-MHz Larmor frequency of3 He gas. The gas is prepared with an optical pumping technique by which energy is transferred by laser to a small quantity of a rubidium agent, which, in turn, conveys it to low-energy-state dipoles of the resident3 He. In healthy individuals,3 He gas is transferred immediately and completely to the most peripheral airways and airspaces because of its high intrinsic diffusibility.[81, 82]
When ventilation defects are observed, healthy areas continue to have a homogeneous distribution. One patient in the de Lange study had a history of asthma and normal findings with initial testing. One week later, when the patient had mild seasonal allergies, repeat examination revealed 2 new, discrete, peripheral ventilation defects when the patient had a new onset of allergic symptoms. The findings subsequently resolved on MRIs obtained 1 week later and after treatment.[83]
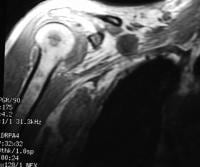
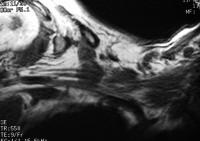
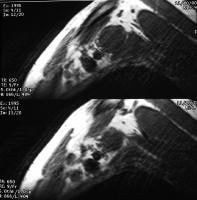
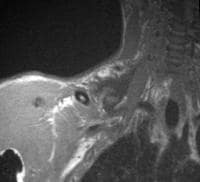
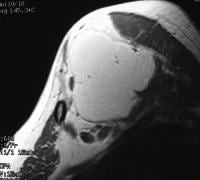
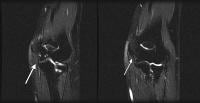
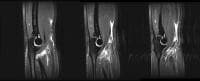
A later study demonstrated similar reversibility in patients receiving the bronchodilator albuterol(see the images below).[84] The proposed mechanism of action is mucous plugging or bronchospasm, although peripheral defects alone are not believed to be unique to asthma, and they also reflect small airway processes such as emphysema, bronchiolitis, and cystic fibrosis.
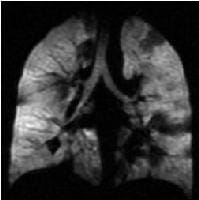 Asthma. Coronal hyperpolarized helium (He-3) MRI in a patient with moderately persistent asthma who underwent imaging twice: This first image was obtained before treatment with an inhaled bronchodilator (ie, albuterol). Multiple dark areas of wedge-shaped ventilation defects improve or resolve after albuterol treatment. Courtesy of T. Altes, MD, and E. de Lange, MD, University of Virginia.
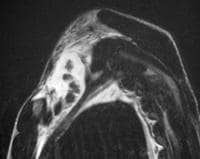
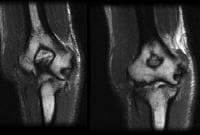
Asthma. Coronal hyperpolarized helium (He-3) MRI in a patient with moderately persistent asthma who underwent imaging twice: This first image was obtained before treatment with an inhaled bronchodilator (ie, albuterol). Multiple dark areas of wedge-shaped ventilation defects improve or resolve after albuterol treatment. Courtesy of T. Altes, MD, and E. de Lange, MD, University of Virginia. 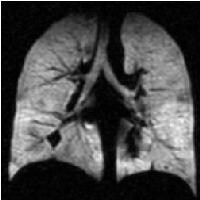 Asthma. Coronal hyperpolarized helium (He-3) MRI in a patient with moderately persistent asthma who underwent imaging twice: This second image was obtained 40 minutes after treatment with an inhaled bronchodilator (ie, albuterol). Multiple dark areas of wedge-shaped ventilation defects improve or resolve after albuterol treatment. The forced expiratory volume in 1 second improved from 83% of the predicted value to 93% after treatment (same patient as in the previous image). Courtesy of T. Altes, MD, and E. de Lange, MD, University of Virginia. In comparison to the results of nuclear medicine ventilation lung scanning with xenon-133 gas, the resolution of ventilation defects on MRIs is substantially superior. Interobserver variability is yet to be tested on a larger scale, but it appeared to be acceptable in the group studied.[83] .[84] Problems related to the availability of the fundamental gas are yet to be overcome, but they may be solved by hyperpolarizing the gas and making slight modifications to the MRI unit.
Asthma. Coronal hyperpolarized helium (He-3) MRI in a patient with moderately persistent asthma who underwent imaging twice: This second image was obtained 40 minutes after treatment with an inhaled bronchodilator (ie, albuterol). Multiple dark areas of wedge-shaped ventilation defects improve or resolve after albuterol treatment. The forced expiratory volume in 1 second improved from 83% of the predicted value to 93% after treatment (same patient as in the previous image). Courtesy of T. Altes, MD, and E. de Lange, MD, University of Virginia. In comparison to the results of nuclear medicine ventilation lung scanning with xenon-133 gas, the resolution of ventilation defects on MRIs is substantially superior. Interobserver variability is yet to be tested on a larger scale, but it appeared to be acceptable in the group studied.[83] .[84] Problems related to the availability of the fundamental gas are yet to be overcome, but they may be solved by hyperpolarizing the gas and making slight modifications to the MRI unit. Additional studies have been performed by using hyperpolarized xenon-129 gas. Oxygen has significant paramagnetic properties and, when used in a 100% concentration, it obviates the use of specialized materials and equipment that is required in3 He hyperpolarized gas. The use of oxygen requires specialization of the pulse sequences, but it is highly diffusible, cheap, and available, and oxygen can be used readily without modifications to the basic MRI unit.
In animal and human studies, Chen et al have shown the effectiveness of centrically reordered single-shot rapid acquisition with relaxation enhancement, a short effective echo time, and short interecho spacing.[85, 86] Oxygen-enhanced MRI techniques also show great promise in functional imaging of the airways.
Ultrasonography
Generally, the use of ultrasonography in chest imaging is limited to the evaluation of mediastinal masses or pleural disease, with or without procedural localization. In airway diseases, the numerous reflective interfaces of the air spaces severely limit the acquisition of diagnostic information. Sonography does not provide truly reproducible images of specific airways that are useful in diagnosis or in monitoring treatment responses. One study of paranasal A-mode ultrasonography compared with radiography recognized the need to screen patients with asthma for correlative sinus disease. The authors found no reliable relationship between use of A-mode ultrasonography and the standard use of plain radiography.[87]Nuclear Imaging
Nuclear medicine technology has been used in the study of aerosol and particulate distribution in the airways. Technetium-99m DTPA radioaerosol lung scintigraphy is a classic technique that shows the extent of major airway distribution, peripheral distribution (depending on particle size), and absorption in the oronasal air passages. Time-activity curves of the radioaerosol have been generated as an index of bronchoalveolar epithelial permeability in asthmatic and nonasthmatic house painters occupationally exposed to isocyanates and have shown a positive correlation between the rate of clearance and work duration.[88]Technetium-99m radioaerosol has been used to show improved peripheral lung distribution of corticosteroid both in normal subjects and in persons treating their asthma using dry-powder inhalers as opposed to pressurized metered-dose inhalers (pMDIs) with a spacer device. One study has shown improved peripheral deposition of inhaled corticosteroid and several measures of lung function after 1 week of pretreatment with a bronchodilator. However, another study showed no significant change in peripheral radioaerosol distribution after 2 months of pMDI administration of corticosteroid with a spacer, despite improvements in FVC and a serum marker of asthmatic inflammation. The authors concluded that improvements in airway function due to aerosolized corticosteroids could occur despite the lack of change in lung deposition.[89, 90, 91, 92]
Ventilation scanning with99m Tc DTPA has also been used as an indicator of ventilation defects in asthmatic children, demonstrating an improvement in homogeneity in distribution of radioaerosol after inhaled steroid therapy. Decreased oral deposition has also been shown with spacer devices and has been linked to a lower prevalence of oral candidiasis and systemic absorption.[93, 94]
The formulation of nonchlorofluorocarbon propellants—namely hydrofluoroalkane (HFA)—has allowed the production of substantially smaller particle size (mass median aerodynamic diameter of 1.2 micrometers rather than the 3.8-micrometer size of the chlorofluorocarbon formulation). This has allowed better drug deposition to the small airways, less oropharyngeal deposition, a low risk of systemic absorption, and small improvements in secondary efficacy measures (eg, as-needed albuterol use, asthma symptoms). Because studies have shown that the inflammatory response in the distal lung in asthma can exceed that in the large airways, the new HFA-based corticosteroids have the potential to treat asthma more effectively and at reduced steroid doses.[95]
In children given a beclomethasone dipropionate/HFA formulation, lung deposition increased with age among groups aged 5-7 years, 8-10 years, and 11-14 years and positively correlated with FEV1 and FVC. The gastrointestinal dose correlated negatively with age, height, and extent of obstructive disease in these subjects. An argument has been put forward that given the difficulty in conducting direct measurements of the clinical responses to inhaled asthma drugs, lung deposition data could be used as a surrogate for the clinical response to new agents. Such data could help save significant time in the drug development process.[96, 97]
While conventional lung scintigraphy has involved the process of physically associating pharmaceuticals in a nebulizer, pMDI, or dry powder form, the physical dissociation of the drug from radioaerosol has limited investigations of drug kinetics. Positron emitters such as carbon-11 and fluorine-18 can be directly incorporated into the drug formulations and then evaluated using positron emission tomography (PET) technology. Not only are 3-dimensional and higher-resolution images possible, but now evaluations of drug uptake and metabolism are possible.[98]
Berridge has (1) demonstrated that central airway (ie, tracheal and major bronchial) deposition of triamcinolone aerosol is demonstrated much better by PET than would have been expected with standard99m Tc planar imaging; (2) demonstrated that a rapid fall-off occurs in the drug formulation due to mucociliary clearance; and (3) estimated that despite the fall-off of radiotracer in the peripheral lung, the therapeutic effects likely relate to the presumably steroid-receptor–rich target. Once again, improved peripheral deposition and reduced oropharyngeal deposition were proven with a spacer device used in drug delivery.[99]
Another use of PET has been in the differentiation of COPD from asthma. Jones et al used 18-fluorodeoxyglucose and carbon-11 PK11195 to show that in situ neutrophil uptake of 18-fluorodeoxyglucose was greater in COPD patients than in normal subjects or those with asthma. Mean uptake of carbon-11 PK11195 into macrophages was mostly greater in both the COPD and asthmatic patients than in control subjects in this pilot study.[100]