To contact us Click HERE
Radiography is an imaging technique that produces high-quality anatomic images by using x-rays. General radiography is currently a major part of hospital imaging departments and includes abdomen, chest and extremity examinations.The use of digital radiography has rapidly increased in recent years. Computed radiography provided a cost-effective transition mode from the traditional film (from the year 1895) to the direct digital radiography (DDR), by using conventional x-ray equipment. Direct digital radiography is a cassette-less imaging system and is ideal for applications where high throughput is of primary importance. The direct digital radiography system should allow usage of all general radiography diagnostic applications.The major components of a digital radiography system are as follows:
1. X-ray generator
2. X-ray assembly
3. Table trolley or other device to support the patient
4. Support for the x-ray tube assembly
5. Detector which converts the x-rays to an image
6. Acquisition workstation to process and display the imageThere is a variety of technologies on which the direct digital radiography is based:
1) Indirect conversion detector: x-rays are converted to light scintillations and light is converted to electric signals.
2) Direct Conversion Detector: x-rays are directly converted to electric signals.
3) Linear Scanning Detectors: A fan beam of x-ray scans the examined area synchronously with a slot of detectors.Due to the structure of the detectors, indirect and direct x-ray conversion detectors are frequently referred to as flat panel detectors (FPD's). There are also portable digital cassettes available, either sold as part of a system or can be retrofitted to an existing CR or film/screen room. Portable detectors can be used in conjunction with an x-ray mobile unit. Such detectors can be connected to a review work station by wire or via a radio link.Most of the digital detectors will need some level of environmental control. This may be in terms of operating temperature range, rate of exchange of temperature and/ or relative humidity.As the original image from the detector is likely to be unsuitable for operating; image processing needs to be applied. A flat field correction is usually applied to the raw image to account for variations in the detector sensitivity across its full area. Also, a number of individual pixels may be defective.The majority of direct digital radiography units are provided with automatic exposure control (AEC) to provide the selected dose to the detector. This may use a conventional AEC detector or the actual image detector to determine the correct dose level. It is essential that the AEC operates in a reliable and consistent manner and that it is correctly set up for the detector of the exposure.Optimization is the process of identifying the necessary radiation dose level to provide adequate clinical information for a particular examination. Optimization depends on a range of both clinical and technical factors.In modern digital radiography systems there is an inbuilt detector dose indicator. The detector dose indicator (DDI) gives an indication of the level of radiation exposure received by the detector. This is useful for monitoring that the exposure is in the correct range for optimal image quality and for undertaking QA.MedWOW.com - an innovative Medical Equipment marketplace for new and used medical equipment. To learn more about Digital Radiography and Medical Radiography Equipment please visit MedWOW.comArticle Source: http://EzineArticles.com/?expert=Bill_Pere
Article Source: http://EzineArticles.com/5396824
25 Haziran 2012 Pazartesi
Diagnostic Radiology - The Advanced Imaging Techniques to Diagnose Fatal Disease
To contact us Click HERE
Diagnostic radiology includes the technique and process that are used to generate images of the human body for the clinical purposes. There are certain medical procedures that are used to reveal, diagnose or examine disease. The imaging of the organs and tissues can be performed as a part of radiotherapy by which the images of the organs and tissues are generated to detect the problem in a better way.
Basically, physicians perform two forms of radiographic images, such as projection radiography and fluoroscopy. These two-dimensional techniques cost low in comparison to the 3D tomography. In the wide sense this biological imaging incorporates radiology, nuclear medicine, endoscopy, investigative radiological sciences, thermography, medical photography and microscopy.
Fluoroscopy generates real-time images of internal structures of the body by employing a constant input of X-rays at a lower dose rate. On the other hand projectional radiographs, known as X-ray, are used to determine the type and extent of the damaged bone or fractures as well as they help to detect pathological changes in the lungs.
There is certain imaging techniques used under the diagnostic radiology. The popular techniques are Magnetic resonance imaging (MRI) scan, Computed tomography (CT) scan, X-ray, Ultrasound. Physicians can use radiographic methods for extensive clinical purposes, such as-
Cardiovascular radiology- it is used to diagnose the diseases of the heart and blood vessels. Physicians perform X-ray, CT, MRI and ultrasound for under this treatment procedure.
Breast imaging- this imaging technology can be used for the diagnosis of breast diseases and conditions. Here doctors can perform mammography, breast ultrasound, breast MRI and breast biopsy to heal breast cancers.
Chest radiology- this stream of radiology is devoted to diagnose the diseases related to chest, such as heart and lung cancers. It takes the help of X-ray, ultrasound, MRI, CT and chest procedures.
Gastrointestinal (GI) radiology- this branch of radiology is used for the imaging and diagnosis of the gastrointestinal (or digestive tract) and abdomen. The CT scan, X-ray, MRI, GI procedures are very useful for such biopsy.
Head and neck radiology- this type of radiology is used for the imaging and diagnosis of the head and neck diseases. It includes several radiographic technologies including CT (or CAT), MRI, ultrasound, X-ray.
There are some other forms of diagnostic radiology, such as emergency radiology, genitourinary radiology, musculoskeletal radiology, neuroradiology, pediatric radiology, interventional radiology, radiation oncology, nuclear radiology, etc.
For more information about radiology, treatment of cancer, diagnostic radiology, and computed tomography please visit radiology-info.org
Article Source: http://EzineArticles.com/?expert=Rebecca_Brown
Article Source: http://EzineArticles.com/3963800
Basically, physicians perform two forms of radiographic images, such as projection radiography and fluoroscopy. These two-dimensional techniques cost low in comparison to the 3D tomography. In the wide sense this biological imaging incorporates radiology, nuclear medicine, endoscopy, investigative radiological sciences, thermography, medical photography and microscopy.
Fluoroscopy generates real-time images of internal structures of the body by employing a constant input of X-rays at a lower dose rate. On the other hand projectional radiographs, known as X-ray, are used to determine the type and extent of the damaged bone or fractures as well as they help to detect pathological changes in the lungs.
There is certain imaging techniques used under the diagnostic radiology. The popular techniques are Magnetic resonance imaging (MRI) scan, Computed tomography (CT) scan, X-ray, Ultrasound. Physicians can use radiographic methods for extensive clinical purposes, such as-
Cardiovascular radiology- it is used to diagnose the diseases of the heart and blood vessels. Physicians perform X-ray, CT, MRI and ultrasound for under this treatment procedure.
Breast imaging- this imaging technology can be used for the diagnosis of breast diseases and conditions. Here doctors can perform mammography, breast ultrasound, breast MRI and breast biopsy to heal breast cancers.
Chest radiology- this stream of radiology is devoted to diagnose the diseases related to chest, such as heart and lung cancers. It takes the help of X-ray, ultrasound, MRI, CT and chest procedures.
Gastrointestinal (GI) radiology- this branch of radiology is used for the imaging and diagnosis of the gastrointestinal (or digestive tract) and abdomen. The CT scan, X-ray, MRI, GI procedures are very useful for such biopsy.
Head and neck radiology- this type of radiology is used for the imaging and diagnosis of the head and neck diseases. It includes several radiographic technologies including CT (or CAT), MRI, ultrasound, X-ray.
There are some other forms of diagnostic radiology, such as emergency radiology, genitourinary radiology, musculoskeletal radiology, neuroradiology, pediatric radiology, interventional radiology, radiation oncology, nuclear radiology, etc.
For more information about radiology, treatment of cancer, diagnostic radiology, and computed tomography please visit radiology-info.org
Article Source: http://EzineArticles.com/?expert=Rebecca_Brown
Article Source: http://EzineArticles.com/3963800
Medical Radiography Careers
To contact us Click HERE
Medical Radiographers are professionals who use complicated imaging apparatus to x-ray various parts of the human body and assist a thorough diagnosis. They execute medical imaging actions to diagnose medical problems. They are also responsible for preparing patients for radiology examinations, positioning them properly under the machines and ensuring accurate doses of radiation. They also have to maintain patient records and radiographic apparatus.
They find employment in medical practitioner offices, clinics, hospitals and diagnostic imaging centers. Their earning ranges from $18.00 to $24.50 per hour. The medical radiography field over the next few years is expected to grow by leaps and bounds. An estimated job opening of 200 vacancies every year is expected. This is because radiography is assuming important proportions in the diagnostic field. It is almost impossible to diagnose a disease without use of radiography.
The American Registry of Radiology Technologists, ARRT, administer certifying exams for Radiology Technologists. In the Arizona State, a certificate from Medical Radiology Technology Board of Examiners (MRTBE) is necessary for employment. Gate Way community college is one of the colleges offering courses in medical radiography. It offers an associate in applied science degree in medical radiography. The degree not only teaches basic imaging principles, but also prepares the student with the job skills necessary for service. After doing a foundation course in medical radiography the student can further advance his career prospects in other imaging professions such as diagnostic medical ultrasound, nuclear medicine technology and magnetic resonance imaging. Apollo College, Colorado Technical University are among many schools and colleges that offer degree or certificate programs resulting in a career as an X Ray technician, Radiographer or a Radiology Technologist.
Thus, medical radiography is a wise career choice today. It ensures recognition in the field of medicine, since no diagnosis is complete without radiographic evidence.
Medical Careers [http://www.e-MedicalCareers.com] provides detailed information on Medical Careers, Top Medical Careers, Medical Billing Careers, Medical Coding Careers and more. Medical Careers is affiliated with Medical Malpractice Law [http://www.e-medicalmalpractice.com].
Article Source: http://EzineArticles.com/?expert=Eric_Morris
Article Source: http://EzineArticles.com/408869
They find employment in medical practitioner offices, clinics, hospitals and diagnostic imaging centers. Their earning ranges from $18.00 to $24.50 per hour. The medical radiography field over the next few years is expected to grow by leaps and bounds. An estimated job opening of 200 vacancies every year is expected. This is because radiography is assuming important proportions in the diagnostic field. It is almost impossible to diagnose a disease without use of radiography.
The American Registry of Radiology Technologists, ARRT, administer certifying exams for Radiology Technologists. In the Arizona State, a certificate from Medical Radiology Technology Board of Examiners (MRTBE) is necessary for employment. Gate Way community college is one of the colleges offering courses in medical radiography. It offers an associate in applied science degree in medical radiography. The degree not only teaches basic imaging principles, but also prepares the student with the job skills necessary for service. After doing a foundation course in medical radiography the student can further advance his career prospects in other imaging professions such as diagnostic medical ultrasound, nuclear medicine technology and magnetic resonance imaging. Apollo College, Colorado Technical University are among many schools and colleges that offer degree or certificate programs resulting in a career as an X Ray technician, Radiographer or a Radiology Technologist.
Thus, medical radiography is a wise career choice today. It ensures recognition in the field of medicine, since no diagnosis is complete without radiographic evidence.
Medical Careers [http://www.e-MedicalCareers.com] provides detailed information on Medical Careers, Top Medical Careers, Medical Billing Careers, Medical Coding Careers and more. Medical Careers is affiliated with Medical Malpractice Law [http://www.e-medicalmalpractice.com].
Article Source: http://EzineArticles.com/?expert=Eric_Morris
Article Source: http://EzineArticles.com/408869
Brain Imaging in Multiple Sclerosis
To contact us Click HERE
Magnetic resonance imaging (MRI) of the brain is useful in the diagnosis and treatment of multiple sclerosis (MS), an inflammatory, demyelinating condition of the central nervous system (CNS) that is generally considered to be autoimmune in nature. White matter tracts are affected, including those of the cerebral hemispheres, infratentorium, and spinal cord. MS lesions, known as plaques, may form in CNS white matter in any location; thus, clinical presentations may be diverse. Continuing lesion formation in MS often leads to physical disability and, sometimes, to cognitive decline.
 Sagittal T1-weighted MRI depicts multiple hypointense lesions in the corpus callosum; this finding is characteristic of multiple sclerosis.
Sagittal T1-weighted MRI depicts multiple hypointense lesions in the corpus callosum; this finding is characteristic of multiple sclerosis.  Coronal fluid-attenuated inversion recovery (FLAIR) MRI in a patient with multiple sclerosis demonstrates periventricular high–signal intensity lesions, which exhibit a typical distribution for multiple sclerosis. FLAIR MRI is a highly sensitive sequence for lesion detection, particularly supratentorially.
Coronal fluid-attenuated inversion recovery (FLAIR) MRI in a patient with multiple sclerosis demonstrates periventricular high–signal intensity lesions, which exhibit a typical distribution for multiple sclerosis. FLAIR MRI is a highly sensitive sequence for lesion detection, particularly supratentorially.  Axial T2-weighted MRI in a patient with multiple sclerosis demonstrates numerous white matter plaques in a callosal and pericallosal white matter distribution.
Axial T2-weighted MRI in a patient with multiple sclerosis demonstrates numerous white matter plaques in a callosal and pericallosal white matter distribution.  Axial diffusion-weighted MRI in a patient with multiple sclerosis shows several hyperintense lesions, a feature of inflammatory disease activity. One of the limitations of using MRI in patients with MS is the discordance occurring between lesion location and the clinical presentation. In addition, depending on the number and location of findings, MRI can vary greatly in terms of sensitivity and specificity in the diagnosis of MS. This is especially true of primary progressive MS, which may not show the classic discrete lesions of relapsing-remitting MS.
Axial diffusion-weighted MRI in a patient with multiple sclerosis shows several hyperintense lesions, a feature of inflammatory disease activity. One of the limitations of using MRI in patients with MS is the discordance occurring between lesion location and the clinical presentation. In addition, depending on the number and location of findings, MRI can vary greatly in terms of sensitivity and specificity in the diagnosis of MS. This is especially true of primary progressive MS, which may not show the classic discrete lesions of relapsing-remitting MS.
A clinician presented with an MRI report that details a few "nonspecific white matter lesions" that are "compatible with MS" is often frustrated with the lack of sensitivity and specificity of such a description. For this reason, imaging findings need to be described in detail, and preferably referenced to one of the published set of diagnostic criteria such as those by Paty[1] or Barkhof.[2] Finally, the specific patient's neurologic history and clinical findings must be correlated with the imaging to establish an accurate diagnosis.[3]
Plain radiographic studies have no positive predictive value in the diagnosis of multiple sclerosis, but occasionally, plain radiographs may be used to exclude mechanical bony lesions. Angiography also has a limited role in the diagnosis and management of MS, but when central nervous system (CNS) vasculitis is considered in a patient with undifferentiated findings, angiography may occasionally be considered.
Cerebrospinal fluid (CSF) analysis for oligoclonal banding or immunoglobulin G (IgG) levels is no longer routine in the investigation of MS, although this test may be of use when MRI is unavailable or MRI findings are nondiagnostic.[4]
Clinically, MS has historically been diagnosed via the demonstration of white matter dysfunction disseminated in time and space.[8] With the advent of diagnostic laboratory investigations and imaging techniques, the Poser criteria were proposed to establish a degree of certainty of diagnosis in the absence of the 2 clinical attacks by using terms such as possible MS and probable MS.[9]
With increasing treatment options for MS and better imaging techniques, newer diagnostic criteria have been suggested that allow diagnosis after a single attack coupled with appropriate positive test results. These criteria have been coined the MacDonald criteria.[10] Essentially, they allow for the second attack in time to be defined by a new lesion appearing on MRI. Also, the MacDonald criteria allow the dissemination in space to be established on the basis of either 9 typical white matter lesions on MRI or 1 enhancing lesion. If CSF studies show increased IgG values or oligoclonal banding, the presence of only 2 typical MRI lesions satisfy the dissemination-in-time criteria.
With respect to the initial clinical presentation in MS, it may vary with the white matter tract involved, and it may include somatic sensory changes, optic neuritis, or weakness, to mention just a few possible neurologic presentations. After only a single attack, the diagnosis of MS is suggested if the first impairment is coupled with positive paraclinical test results, such as those on imaging or CSF studies. Furthermore, the attack must be compatible with the pattern of impairment found in patients with MS, which typically means that the duration of deficit is days to weeks. Worsening of vision due to optic neuritis and subsequent exercise is known as the Uhthoff phenomenon.
Stankiewicz et al correlated brain lesions and clinical status with 1.5T and 3T MRI in 32 patients with MS by use of MRI fluid-attenuated inversion-recovery (FLAIR) sequences, and the authors found that MRI at 3T may provide increased sensitivity and validity in assessment of MS brain lesions. The study showed that FLAIR lesion volume (FLLV) at 3T was higher than at 1.5T. While 3T FLLV correlated moderately and significantly, 1.5T FLLV correlated poorly. When controlling for age and depression, correlations between FLLV and cognitive measures were significant at 1.5T for the Judgment of Line Orientation Test, the Symbol Digit Modalities Test, and the California Verbal Learning Test Delayed Free Recall, but at 3T, correlations were significant and of greater magnitude.[11]
Occasionally, the course of MS may be more indolent and exhibit a chronic, persistent neurologic deficit without apparent ongoing deterioration or further impairment. Sometimes, this course of MS is called inactive or benign MS, and this form is often observed in patients with prior relapsing-remitting disease.
Another potentially complicating matter clinically is that highly active MS lesions may sometimes demonstrate significant mass effect. Rarely, mass effect can lead to midline shift, herniations, infarctions, and even death. Such a drastic clinical and radiologic presentation can lead to an incorrect preliminary diagnosis and inappropriate neurosurgical intervention. When MS presents in a more fulminant, aggressive manner, it is frequently known as malignant MS or the Marburg variant.
In a prospective study, Lebrun et al followed 70 patients who had their first brain MRI for a variety of medical symptoms not suggestive of MS and found the mean time between the first brain MRI and the first clinically isolated syndrome to be 2.3 years (range, 0.8-5 y). Diagnostic studies of the blood, CSF, and visual evoked potentials were conducted, and clinical conversion occurred in 23 patients: 6 to optic neuritis, 6 to myelitis, 5 to brainstem symptoms, 4 to sensitive symptoms, 1 to cerebellar symptoms, and 1 to cognitive deterioration.[12] For patient education information, see Multiple Sclerosis.
Preferred examination
Radiologically, the use of MRI is revolutionizing the investigation, diagnosis, and even the treatment of MS (see the images below). Usually, MRI is the only imaging modality needed for imaging patients with MS, and it far surpasses all other tests with respect to its positive predictive value.Sagittal T1-weighted MRI depicts multiple hypointense lesions in the corpus callosum; this finding is characteristic of multiple sclerosis. Coronal fluid-attenuated inversion recovery (FLAIR) MRI in a patient with multiple sclerosis demonstrates periventricular high–signal intensity lesions, which exhibit a typical distribution for multiple sclerosis. FLAIR MRI is a highly sensitive sequence for lesion detection, particularly supratentorially. Axial T2-weighted MRI in a patient with multiple sclerosis demonstrates numerous white matter plaques in a callosal and pericallosal white matter distribution. Axial diffusion-weighted MRI in a patient with multiple sclerosis shows several hyperintense lesions, a feature of inflammatory disease activity. One of the limitations of using MRI in patients with MS is the discordance occurring between lesion location and the clinical presentation. In addition, depending on the number and location of findings, MRI can vary greatly in terms of sensitivity and specificity in the diagnosis of MS. This is especially true of primary progressive MS, which may not show the classic discrete lesions of relapsing-remitting MS.A clinician presented with an MRI report that details a few "nonspecific white matter lesions" that are "compatible with MS" is often frustrated with the lack of sensitivity and specificity of such a description. For this reason, imaging findings need to be described in detail, and preferably referenced to one of the published set of diagnostic criteria such as those by Paty[1] or Barkhof.[2] Finally, the specific patient's neurologic history and clinical findings must be correlated with the imaging to establish an accurate diagnosis.[3]
Plain radiographic studies have no positive predictive value in the diagnosis of multiple sclerosis, but occasionally, plain radiographs may be used to exclude mechanical bony lesions. Angiography also has a limited role in the diagnosis and management of MS, but when central nervous system (CNS) vasculitis is considered in a patient with undifferentiated findings, angiography may occasionally be considered.
Cerebrospinal fluid (CSF) analysis for oligoclonal banding or immunoglobulin G (IgG) levels is no longer routine in the investigation of MS, although this test may be of use when MRI is unavailable or MRI findings are nondiagnostic.[4]
Clinical diagnosis
A diagnosis of MS is made on the basis of clinical findings by using supporting evidence from ancillary tests such as CSF examination for oligoclonal banding and MRI.[5, 6, 7]Clinically, MS has historically been diagnosed via the demonstration of white matter dysfunction disseminated in time and space.[8] With the advent of diagnostic laboratory investigations and imaging techniques, the Poser criteria were proposed to establish a degree of certainty of diagnosis in the absence of the 2 clinical attacks by using terms such as possible MS and probable MS.[9]
With increasing treatment options for MS and better imaging techniques, newer diagnostic criteria have been suggested that allow diagnosis after a single attack coupled with appropriate positive test results. These criteria have been coined the MacDonald criteria.[10] Essentially, they allow for the second attack in time to be defined by a new lesion appearing on MRI. Also, the MacDonald criteria allow the dissemination in space to be established on the basis of either 9 typical white matter lesions on MRI or 1 enhancing lesion. If CSF studies show increased IgG values or oligoclonal banding, the presence of only 2 typical MRI lesions satisfy the dissemination-in-time criteria.
With respect to the initial clinical presentation in MS, it may vary with the white matter tract involved, and it may include somatic sensory changes, optic neuritis, or weakness, to mention just a few possible neurologic presentations. After only a single attack, the diagnosis of MS is suggested if the first impairment is coupled with positive paraclinical test results, such as those on imaging or CSF studies. Furthermore, the attack must be compatible with the pattern of impairment found in patients with MS, which typically means that the duration of deficit is days to weeks. Worsening of vision due to optic neuritis and subsequent exercise is known as the Uhthoff phenomenon.
Stankiewicz et al correlated brain lesions and clinical status with 1.5T and 3T MRI in 32 patients with MS by use of MRI fluid-attenuated inversion-recovery (FLAIR) sequences, and the authors found that MRI at 3T may provide increased sensitivity and validity in assessment of MS brain lesions. The study showed that FLAIR lesion volume (FLLV) at 3T was higher than at 1.5T. While 3T FLLV correlated moderately and significantly, 1.5T FLLV correlated poorly. When controlling for age and depression, correlations between FLLV and cognitive measures were significant at 1.5T for the Judgment of Line Orientation Test, the Symbol Digit Modalities Test, and the California Verbal Learning Test Delayed Free Recall, but at 3T, correlations were significant and of greater magnitude.[11]
Clinical course
The clinical course of MS can follow different patterns, and this observation has led to the classification of distinct types of MS. The most common form of MS is termed relapsing-remitting MS, in which progression involves symptoms of neurologic dysfunction frequently followed by partial or complete clinical recovery. In relapsing-remitting MS, global clinical deterioration has traditionally been attributed to cumulative deficit due to incomplete recovery from repeated occurrences of individual relapses. However, this cumulative deficit has been questioned, because evidence increasingly suggests an ongoing background neurologic deterioration that is independent of the relapses.Occasionally, the course of MS may be more indolent and exhibit a chronic, persistent neurologic deficit without apparent ongoing deterioration or further impairment. Sometimes, this course of MS is called inactive or benign MS, and this form is often observed in patients with prior relapsing-remitting disease.
Another potentially complicating matter clinically is that highly active MS lesions may sometimes demonstrate significant mass effect. Rarely, mass effect can lead to midline shift, herniations, infarctions, and even death. Such a drastic clinical and radiologic presentation can lead to an incorrect preliminary diagnosis and inappropriate neurosurgical intervention. When MS presents in a more fulminant, aggressive manner, it is frequently known as malignant MS or the Marburg variant.
In a prospective study, Lebrun et al followed 70 patients who had their first brain MRI for a variety of medical symptoms not suggestive of MS and found the mean time between the first brain MRI and the first clinically isolated syndrome to be 2.3 years (range, 0.8-5 y). Diagnostic studies of the blood, CSF, and visual evoked potentials were conducted, and clinical conversion occurred in 23 patients: 6 to optic neuritis, 6 to myelitis, 5 to brainstem symptoms, 4 to sensitive symptoms, 1 to cerebellar symptoms, and 1 to cognitive deterioration.[12] For patient education information, see Multiple Sclerosis.
The New York Review of Books: Someone Else's Children
To contact us Click HERE
The Burns Archive is pleased to announce our exhibition Reed Bontecou: Masterpieces of Civil War Portraiture and accompanying publication Shooting Soldiers have been covered by The New York Review of Books:

Someone Else’s Children
Christopher Benfey
November 28, 2011
My wife and I have two sons, aged eighteen and twenty-two. Both have registered for the Selective Service, as the law requires. (“Our objective is to register you,” the official letter reminded them, “not to have you prosecuted.”) We don’t have a clear idea of Tommy’s or Nicholas’s views regarding military service; we hope that circumstances won’t force us to find out. None of us knows any men or women currently serving in Iraq or Afghanistan. They are someone else’s children. We watch news reports of wounded veterans learning to walk with prosthetic limbs. Recent stories about body parts mislaid at the military mortuary at Dover Air Force Base fill us with outrage. Still, for many of us, it is a general, not an individualized outrage.
During the Civil War, in contrast, the mangling of young bodies was evident to all. Three million volunteers armed with advanced rifles, and firing at one another at point-blank range, fought on battlefields often not far from their own homes. American writers, many of whom had children in the war, were not insulated from the carnage. Fred Stowe was standing in the graveyard on Cemetery Ridge, above Gettysburg, when a live shell exploded near his ear, opening a wound that never healed. Charles Longfellow sought distraction from the trauma of the war in Yokohama, where he had a giant carp tattooed across his back, around the scars of two bullet holes. Emily Dickinson chose as her literary advisor a Union colonel suffering from PTSD: “We can find no scar,” she wrote in a famous poem, “But internal difference— / Where the Meanings, are.”
Louisa May Alcott and Walt Whitman served as nurses and eyewitness reporters in the hideous Union hospitals in Washington, D. C. Alcott contracted typhoid in the septic wards and wrote Little Women, about the daughters of a father wounded in the war, while treating herself with mercury. Whitman ministered to the needs of wounded soldiers while also keeping a careful visual record of everything he saw, “this other freight of helpless worn and wounded youth,” as he wrote to Emerson. “Doctors sawed arms & legs off from morning till night,” he reported in his journal. He was dismayed to see “a heap of feet, arms, legs, etc., under a tree in front of a hospital.” As he moved from bed to bed in the overcrowded wards, he was shocked by the youth of the victims. “Charles Miller, bed 19, company D, 53rd Pennsylvania, is only sixteen years of age, very bright, courageous boy, left leg amputated below the knee.”
The remarkable medical photographs of the Civil War surgeon-photographer Reed Bontecou—now published in their entirety for the first time and recently shown at The Robert Anderson gallery in New York—bring us closer still. Bontecou, from Troy, New York, was a classifier of seashells and an ornithologist who had traveled in the Amazon before the war collecting specimens. A pioneer in surgical procedures known for the dexterity and speed of his operations, he was also a photographer of genius. His iconic image, “A Morning’s Work,” shows a pile of amputated legs he himself had sawed off earlier that day. Bontecou’s albums served many ends, most obviously instruction, with before-and-after shots, in the identification and treatment of conditions like gangrene and bullets lodged in bone. But they also aided in the later identification of veterans for disbursement of disability and pension funds. Bontecou was apparently an engaging and capable administrator of army hospitals who was once threatened with disciplinary action for inviting a recovering Confederate officer to his home for Thanksgiving dinner.
Most poignant and painful is Bontecou’s artistic ability to capture the terror of his patients, what the editor and collector of medical photographs Stanley Burns, M.D., calls “individual bereavement.” Pvt. John Parmenter, unbearably young, lies prone on an army cot with his beautiful and vulnerable face turned towards us and his gangrenous foot propped up on a cushion. Then, in another photograph, we see him lying deathly pale and unconscious; a surgeon with his hand on one of Parmenter’s bent knees looks down thoughtfully at the severed foot. The picture has some of the bleak, geometrical power of Jacques-Louis David’s Death of Marat.
In another arresting image, Robert Fryer, eighteen years old and wearing his cap and uniform, all gold buttons carefully buttoned, holds his hand to his chest as though playfully mimicking a handgun. His features are deadpan. At first, we assume his hand is partially hidden in his jacket. But no, it’s an illusion, presumably deliberate on the part of the photographer. Fryer’s middle, ring, and little fingers are amputated. According to Bontecou’s notes, “Patient has good use of forefinger and thumb.” Perhaps he watched young Robert Fryer buttoning his coat.
The photographs are a bitter reminder of the hideous race between better medical response and ever more devastating weaponry. If, as Burns notes, the improvised explosive device (IED) has changed the way war is fought and the wounded treated today, the novelty of the Crimean War and the Civil War was the 58 caliber Minie Ball, named for its inventor, Claude-Etienne Minié. This was a war in which 94% of Union wounds were caused by bullets. The Minie Ball, Burns remarks, “shattered and fractured bone easily and commonly carried clothing and other debris with it into the wound, making infection a constant companion in almost every case.” Bontecou’s images “documented the battle against gunshot wounds,” at a time when battle armor was minimal or absent and two years before the discovery of the principles of antiseptic surgery in 1867. Burns adds grimly, “Many of the men we see here are going to die.”
There is another race on display in these photographs, between the sheer horror of the army hospital and our ability to find words and images adequate to the horror. “The real war,” Whitman wrote in Specimen Days, “will never get in the books.” The simple identification boards that many of Bontecou’s patients hold in their hands, with their name and company inscribed in white chalk, carry their own dire and individualized lyricism, as though to say, in Whitman’s resonant words: “I am the man, I suffered, I was there.” Andsell H. Beam, shot in the skull on April 6th, 1865, bows over his identification board as though in prayer, or in simple disbelief in his unfathomable fate. “Now that I have lived for 8 or 9 days amid such scenes as the camps furnish,” Whitman wrote his mother, “… really nothing we call trouble seems worth talking about.”
Shooting Soldiers: Civil War Medical Photography By R.B. Bontecou by Dr. Stanley M. Burns has recently been published.

Someone Else’s Children
Christopher Benfey
November 28, 2011
My wife and I have two sons, aged eighteen and twenty-two. Both have registered for the Selective Service, as the law requires. (“Our objective is to register you,” the official letter reminded them, “not to have you prosecuted.”) We don’t have a clear idea of Tommy’s or Nicholas’s views regarding military service; we hope that circumstances won’t force us to find out. None of us knows any men or women currently serving in Iraq or Afghanistan. They are someone else’s children. We watch news reports of wounded veterans learning to walk with prosthetic limbs. Recent stories about body parts mislaid at the military mortuary at Dover Air Force Base fill us with outrage. Still, for many of us, it is a general, not an individualized outrage.
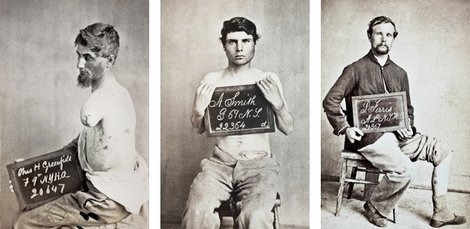 |
| R.B. Bontencou, Courtesey of Stanley B. Burns, MD Charles H. Greenfield (left), wounded April 2, 1865 at Petersberg, VA; A. Smith (center), wounded April 16, 1864 at Southside Railroad; P. Ferris (right), gunshot wound, left leg. |
During the Civil War, in contrast, the mangling of young bodies was evident to all. Three million volunteers armed with advanced rifles, and firing at one another at point-blank range, fought on battlefields often not far from their own homes. American writers, many of whom had children in the war, were not insulated from the carnage. Fred Stowe was standing in the graveyard on Cemetery Ridge, above Gettysburg, when a live shell exploded near his ear, opening a wound that never healed. Charles Longfellow sought distraction from the trauma of the war in Yokohama, where he had a giant carp tattooed across his back, around the scars of two bullet holes. Emily Dickinson chose as her literary advisor a Union colonel suffering from PTSD: “We can find no scar,” she wrote in a famous poem, “But internal difference— / Where the Meanings, are.”
 |
| R.B. Bontencou, Courtesey of Stanley B. Burns, MD “A Morning’s Work” R. B. Bontecou’s label for his iconic image of wartime labors, 1865. |
Louisa May Alcott and Walt Whitman served as nurses and eyewitness reporters in the hideous Union hospitals in Washington, D. C. Alcott contracted typhoid in the septic wards and wrote Little Women, about the daughters of a father wounded in the war, while treating herself with mercury. Whitman ministered to the needs of wounded soldiers while also keeping a careful visual record of everything he saw, “this other freight of helpless worn and wounded youth,” as he wrote to Emerson. “Doctors sawed arms & legs off from morning till night,” he reported in his journal. He was dismayed to see “a heap of feet, arms, legs, etc., under a tree in front of a hospital.” As he moved from bed to bed in the overcrowded wards, he was shocked by the youth of the victims. “Charles Miller, bed 19, company D, 53rd Pennsylvania, is only sixteen years of age, very bright, courageous boy, left leg amputated below the knee.”
 |
| R.B. Bontencou, Courtesey of Stanley B. Burns, MD Pvt. John Parmenter, before being operated on for gangrene. Wounded at Amelia Springs, VA, April 3, 1865 |
The remarkable medical photographs of the Civil War surgeon-photographer Reed Bontecou—now published in their entirety for the first time and recently shown at The Robert Anderson gallery in New York—bring us closer still. Bontecou, from Troy, New York, was a classifier of seashells and an ornithologist who had traveled in the Amazon before the war collecting specimens. A pioneer in surgical procedures known for the dexterity and speed of his operations, he was also a photographer of genius. His iconic image, “A Morning’s Work,” shows a pile of amputated legs he himself had sawed off earlier that day. Bontecou’s albums served many ends, most obviously instruction, with before-and-after shots, in the identification and treatment of conditions like gangrene and bullets lodged in bone. But they also aided in the later identification of veterans for disbursement of disability and pension funds. Bontecou was apparently an engaging and capable administrator of army hospitals who was once threatened with disciplinary action for inviting a recovering Confederate officer to his home for Thanksgiving dinner.
 |
| R.B. Bontencou, Courtesey of Stanley B. Burns, MD Pvt. John Parmenter lying unconscious from anesthesia on operating table with his severed foot, 1865. |
Most poignant and painful is Bontecou’s artistic ability to capture the terror of his patients, what the editor and collector of medical photographs Stanley Burns, M.D., calls “individual bereavement.” Pvt. John Parmenter, unbearably young, lies prone on an army cot with his beautiful and vulnerable face turned towards us and his gangrenous foot propped up on a cushion. Then, in another photograph, we see him lying deathly pale and unconscious; a surgeon with his hand on one of Parmenter’s bent knees looks down thoughtfully at the severed foot. The picture has some of the bleak, geometrical power of Jacques-Louis David’s Death of Marat.
 |
| R.B. Bontencou, Courtesey of Stanley B. Burns, MD Robert Fryer, Private, Age 18. Gunshot wound, right hand. Wounded March 25, 1865, at Battle of Hatcher’s Run. |
The photographs are a bitter reminder of the hideous race between better medical response and ever more devastating weaponry. If, as Burns notes, the improvised explosive device (IED) has changed the way war is fought and the wounded treated today, the novelty of the Crimean War and the Civil War was the 58 caliber Minie Ball, named for its inventor, Claude-Etienne Minié. This was a war in which 94% of Union wounds were caused by bullets. The Minie Ball, Burns remarks, “shattered and fractured bone easily and commonly carried clothing and other debris with it into the wound, making infection a constant companion in almost every case.” Bontecou’s images “documented the battle against gunshot wounds,” at a time when battle armor was minimal or absent and two years before the discovery of the principles of antiseptic surgery in 1867. Burns adds grimly, “Many of the men we see here are going to die.”
 |
| R.B. Bontencou, Courtesey of Stanley B. Burns, MD Andsell H. Beam, Age 24. Gunshot wound to head. Wounded April 6, 1865, Battle Of Farmville, VA. |
Shooting Soldiers: Civil War Medical Photography By R.B. Bontecou by Dr. Stanley M. Burns has recently been published.
24 Haziran 2012 Pazar
I'm back, with good news
To contact us Click HERE
I know I've been gone a while. I won't count off the months and days.
My father-in-law passed away after my last post. Cancer is a terrible thing. It was his second bout with the disease and, sadly, he went undiagnosed until Stage IV the second time around. Chemotherapy gave him some extra time but it didn't seem to be enough. I really miss Bill, and I always will.
On the way home from his funeral ceremony, which was delayed a few weeks for the Christmas holidays, I got the news that my mother was taking a turn for the worse. I flew out and drove straight to her beside getting there just hours before she drifted off into a coma. I never did get to talk to her in any meaningful sense, but that has defined our relationship for 36 years. I think its more difficult to lose a parent you weren't close to sometimes, at least initially. I spent the rest of my trip fighting an adrenal crisis that wouldn't let go.
Meanwhile the surgeon that will be performing my pituitary procedure insisted that I undergo an Inferior Petrosal Sinus Sampling. That's fine, as it assists him when mapping out an approach for surgery. However, arranging for the IPSS was another story. It took from the beginning of January until March 28th to have it scheduled, confirmed and carried out. Then another three weeks for informal results, four weeks for the official ones with a report.
I am happy to say that I do have a date for surgery: May 24th and I do have hope that this Christmas I'll feel better.
I seem to tick off years at Christmas, thinking 'Last year I thought I'd be better by now'. Maybe this is my year.
My father-in-law passed away after my last post. Cancer is a terrible thing. It was his second bout with the disease and, sadly, he went undiagnosed until Stage IV the second time around. Chemotherapy gave him some extra time but it didn't seem to be enough. I really miss Bill, and I always will.
On the way home from his funeral ceremony, which was delayed a few weeks for the Christmas holidays, I got the news that my mother was taking a turn for the worse. I flew out and drove straight to her beside getting there just hours before she drifted off into a coma. I never did get to talk to her in any meaningful sense, but that has defined our relationship for 36 years. I think its more difficult to lose a parent you weren't close to sometimes, at least initially. I spent the rest of my trip fighting an adrenal crisis that wouldn't let go.
Meanwhile the surgeon that will be performing my pituitary procedure insisted that I undergo an Inferior Petrosal Sinus Sampling. That's fine, as it assists him when mapping out an approach for surgery. However, arranging for the IPSS was another story. It took from the beginning of January until March 28th to have it scheduled, confirmed and carried out. Then another three weeks for informal results, four weeks for the official ones with a report.
I am happy to say that I do have a date for surgery: May 24th and I do have hope that this Christmas I'll feel better.
I seem to tick off years at Christmas, thinking 'Last year I thought I'd be better by now'. Maybe this is my year.
Damn you, Cushing's Disease
To contact us Click HERE
How to disappoint all of your friends, relatives and two young children: Spend a month recuperating from pituitary surgery in June - and not have your remission stick. In September I realized that the Cushing's had returned, if it ever left, and I'm just now ready to admit to it.
Thankfully the road is paved already and my specialist is recommending a repeat surgery. Tomorrow I go in for a pituitary MRI and with any luck we can find the source. The abdominal MRI from two weeks ago shows normal adrenal glands. In a twisted way I was hoping that my adrenals were the culprit, even though it goes against all likelihood. Removing the adrenal glands would almost certainly put an end to the Cushing's misery. I'd take Addison's back with a warm heart, since my weight has ballooned beyond all recognition. (I avoid mirrors.) They discovered a cyst on my spleen and liver during the abdominal MRI. No one has addressed those findings, so I don't know what to make of it. A quick Google tells me that it is rare, ha - who knew?, and LORD HELP ME, I now know what 'non-parasitic' means. *la la la la la la* (fingers in ears)
I have some more blood testing to do at midnight, which runs a close second to my most despised form of testing torture, and the MRI tomorrow. As far as symptoms go, weight gain - cystic 'steroid' acne - flank pain - and very recently a deterioration of the vision in my left eye (again). The double vision is slight and I only get migraines once a week or so. My bout with constant 24 hour a day headache & migraine has ruined my ability to describe pain. I cannot fathom calling the first surgery a 'failure', since it single-handedly took away the constant headache.
I'm rambling and it is late.... I'll be back with MRI results soon.
Thankfully the road is paved already and my specialist is recommending a repeat surgery. Tomorrow I go in for a pituitary MRI and with any luck we can find the source. The abdominal MRI from two weeks ago shows normal adrenal glands. In a twisted way I was hoping that my adrenals were the culprit, even though it goes against all likelihood. Removing the adrenal glands would almost certainly put an end to the Cushing's misery. I'd take Addison's back with a warm heart, since my weight has ballooned beyond all recognition. (I avoid mirrors.) They discovered a cyst on my spleen and liver during the abdominal MRI. No one has addressed those findings, so I don't know what to make of it. A quick Google tells me that it is rare, ha - who knew?, and LORD HELP ME, I now know what 'non-parasitic' means. *la la la la la la* (fingers in ears)
I have some more blood testing to do at midnight, which runs a close second to my most despised form of testing torture, and the MRI tomorrow. As far as symptoms go, weight gain - cystic 'steroid' acne - flank pain - and very recently a deterioration of the vision in my left eye (again). The double vision is slight and I only get migraines once a week or so. My bout with constant 24 hour a day headache & migraine has ruined my ability to describe pain. I cannot fathom calling the first surgery a 'failure', since it single-handedly took away the constant headache.
I'm rambling and it is late.... I'll be back with MRI results soon.
Kaydol:
Kayıtlar (Atom)